- 32 scientific abstracts reflect ongoing commitment to improving outcomes for people living with epilepsies
- Data include the use of FINTEPLA® (fenfluramine)1 oral solution in seizures associated with Dravet syndrome and Lennox-Gastaut syndrome, BRIVIACT® (brivaracetam) CV2 and VIMPAT® (lacosamide) CV3 in focal-onset seizures, and *Staccato[®] alprazolam4 (investigational treatment) for acute on-demand seizure management, plus latest updates from UCB’s pipeline programs
- Additional focus on the impact of epilepsy on aspects of everyday life, including research exploring epilepsy and sleep, epilepsy and motherhood, and the consequences of prolonged seizures on the quality of life of patients and caregivers
ATLANTA, GA, November 26, 2024 – 7:00 AM (ET) – UCB today announced it will present 32 abstracts from its expansive epilepsies research program at the American Epilepsy Society (AES) Annual Meeting, December 6-10, 2024 (Los Angeles, California). The data will include clinical and real-world data, plus medical research from across UCB’s pipeline programs.
Dr Dimitrios Bourikas, Global Medical Head of Epilepsy, UCB, commented: “We are excited to share our latest epilepsy research during the American Epilepsy Society Annual Meeting. It’s an honor to connect with the brightest minds working in this field and discuss innovative approaches with the common goal of improving treatment and care. Working together, we strive to address areas of unmet need that impact the lives of people living with epilepsies and those that support them.”
Highlights focus of data to be presented at American Epilepsy Society (AES) Annual Meeting:
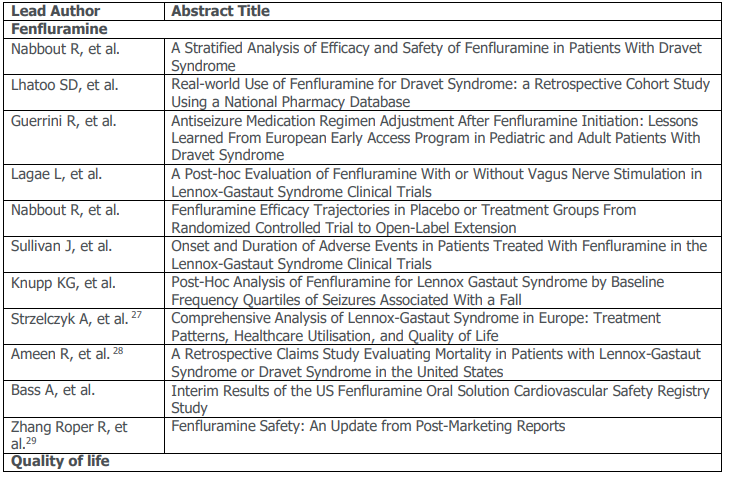
- Dravet syndrome: data include an analysis of the safety and efficacy of fenfluramine5, an assessment of real-world evidence from a retrospective cohort study using a national pharmacy database6 and data from the European early access program assessing medication regimen adjustments in children and adults.7
- Lennox-Gastaut syndrome: post-hoc analyses include an evaluation of the treatment with and without vagus nerve stimulation8, an assessment of efficacy trajectories from the randomized controlled trials to the open label extension study, plus analyses of the onset and duration of adverse events reported with fenfluramine treatment10 and treatment outcomes related to the baseline frequencies of seizures associated with falls.11,12
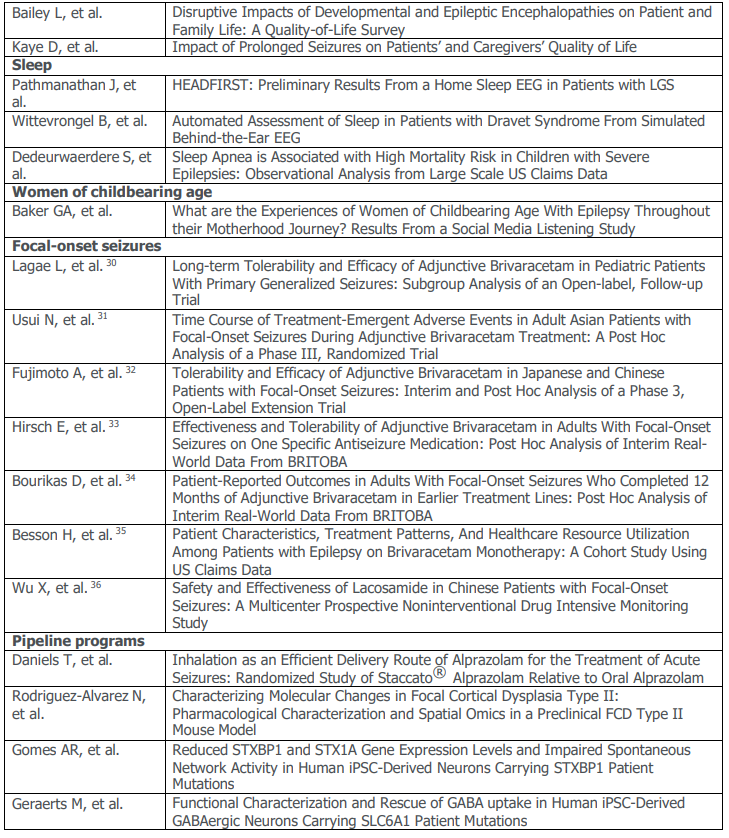
- Quality of life: data include a survey evaluating the disruptive impact of developmental and epileptic encephalopathies on patients’ and families’ quality of life13, and a study exploring the impact of prolonged seizures on patients’ and caregivers’ quality of life.14
- Sleep: data focus on the relationship between sleep and epilepsy, including assessments of a home sleep EEG in patients with LGS15, the use of a simulated behind-the-ear EEG in DS16, and an observational analysis from large scale US claims data of high mortality risk of sleep apnea in children and young adultswith uncontrolled epilepsies.17
- Focal-onset seizures: data include brivaracetam long-term clinical outcomes in pediatric patients with primary generalized seizures25, healthcare resource utilization of brivaracetam monotherapy30, real world experience on use of brivaracetam in earlier treatment lines29 and in combination with one specific antiseizure medication.28
- Women of childbearing age: data include results of a social listening analysis on the experiences and challenges of women living with epilepsy during their motherhood journey.18
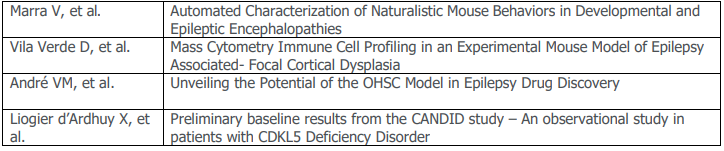
- UCB pipeline: includes data on investigational therapy Staccato[®] alprazolam19, and several studies also assess the molecular, cellular and genetic roots of epilepsies, providing potential avenues for future exploration and drug discovery.20-26
This meeting brings us all together as we explore the vast landscape of research and innovations in the epilepsy space. By harnessing a rich array of data, we drive forward our commitment to the communities we have served for over 30 years now. Our vision is clear: a future where each discovery is a step closer to a world without seizures and the non-seizure impacts of epilepsy and rare epilepsy syndromes such as Dravet and Lennox-Gastaut,” said Brad Chapman, Head of U.S. Epilepsy and Rare Syndromes.
UCB presentations during the American Epilepsy Society Annual Meeting
*The safety and efficacy of Staccato® alprazolam have not been established and it is not currently approved for use in this indication by any regulatory authority worldwide.
For further information, contact UCB:
Corporate Communications
Becky Malone, U.S. Media Relations
T +919.605.9600
Email Becky.Malone@ucb.com
Investor Relations
Antje Witte
T +32.2.559.94.14
Email antje.witte@ucb.com
About UCB
UCB, Brussels, Belgium (www.ucb.com) is a global biopharmaceutical company focused on the discovery and development of innovative medicines and solutions to transform the lives of people living with severe diseases of the immune system or of the central nervous system. With approximately 8,600 people in approximately 40 countries, the company generated revenue of €5.5 billion in 2022. UCB is listed on Euronext Brussels (symbol: UCB). Follow us on Twitter: @UCBUSA
Important Safety Information about FINTEPLA® (fenfluramine) in the US1
FINTEPLA is indicated for the treatment of seizures associated with Dravet syndrome (DS) and Lennox-Gastaut syndrome (LGS) in patients 2 years of age and older.
FINTEPLA is available only through a restricted distribution program called the FINTEPLA REMS. Further information is available at www.FinteplaREMS.com or by telephone at +1 877 964 3649.
IMPORTANT SAFETY INFORMATION
BOXED WARNING: VALVULAR HEART DISEASE and PULMONARY ARTERIAL HYPERTENSION
- There is an association between serotonergic drugs with 5-HT2B receptor agonist activity,
including fenfluramine (the active ingredient in FINTEPLA), and valvular heart disease and
pulmonary arterial hypertension. - Echocardiogram assessments are required before, during, and after treatment with
FINTEPLA. - FINTEPLA is available only through a restricted program called the FINTEPLA REMS.
CONTRAINDICATIONS
FINTEPLA is contraindicated in patients with hypersensitivity to fenfluramine or any of the excipients in FINTEPLA and with concomitant use, or within 14 days of the administration, of monoamine oxidase inhibitors because of an increased risk of serotonin syndrome.
WARNINGS AND PRECAUTIONS
Valvular Heart Disease and Pulmonary Arterial Hypertension (see Boxed Warning): Because of the association between serotonergic drugs with 5-HT2B receptor agonist activity, including fenfluramine (the active ingredient in FINTEPLA), and valvular heart disease (VHD) and pulmonary arterial hypertension (PAH), cardiac monitoring via echocardiogram is required prior to starting treatment, during treatment, and after treatment with FINTEPLA concludes. Cardiac monitoring via echocardiogram can aid in early detection of these conditions. In clinical trials for DS and LGS of up to 3 years in duration, no patient receiving FINTEPLA developed VHD or PAH.
Monitoring: Prior to starting treatment, patients must undergo an echocardiogram to evaluate for VHD and PAH. Echocardiograms should be repeated every 6 months, and once at 3-6 months post treatment with FINTEPLA.
The prescriber must consider the benefits versus the risks of initiating or continuing treatment with FINTEPLA if any of the following signs are observed via echocardiogram: valvular abnormality or new abnormality; VHD indicated by mild or greater aortic regurgitation or moderate or greater mitral regurgitation, with additional characteristics of VHD (eg, valve thickening or restrictive valve motion); PAH indicated by elevated right heart/pulmonary artery pressure (PASP >35 mmHg).
FINTEPLA REMS Program (see Boxed Warning): FINTEPLA is available only through a restricted distribution program called the FINTEPLA Risk Evaluation and Mitigation Strategy (REMS) Program. Prescribers must be certified by enrolling in the FINTEPLA REMS. Prescribers must counsel patients receiving FINTEPLA about the risk of VHD and PAH, how to recognize signs and symptoms of VHD and PAH, the need for baseline (pretreatment) and periodic cardiac monitoring via echocardiogram during FINTEPLA treatment, and cardiac
monitoring after FINTEPLA treatment. Patients must enroll in the FINTEPLA REMS and comply with ongoing monitoring requirements. The pharmacy must be certified by enrolling in the FINTEPLA REMS and must only dispense to patients who are authorized to receive FINTEPLA. Wholesalers and distributors must only distribute to certified pharmacies. Further information is available at www.FinteplaREMS.com or by telephone at 1-877-964-3649.
Decreased Appetite and Decreased Weight: FINTEPLA can cause decreases in appetite and weight. Decreases in weight appear to be dose related. Approximately half of the patients with LGS and most patients with DS resumed the expected measured increases in weight during the open-label extension studies. Weight should be monitored regularly during treatment with FINTEPLA, and dose modifications should be considered if a decrease in weight is observed.
Somnolence, Sedation, and Lethargy: FINTEPLA can cause somnolence, sedation, and lethargy. Other central nervous system (CNS) depressants, including alcohol, could potentiate these effects of FINTEPLA. Prescribers should monitor patients for somnolence and sedation and should advise patients not to drive or operate machinery until they have gained sufficient experience on FINTEPLA to gauge whether it adversely affects their ability to drive or operate machinery.
Suicidal Behavior and Ideation: Antiepileptic drugs (AEDs), including FINTEPLA, increase the risk of suicidal thoughts or behaviors in patients taking these drugs for any indication. Patients treated with an AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behaviors, or any unusual changes in mood or behavior.
Anyone considering prescribing FINTEPLA or any other AED must balance the risk of suicidal thoughts or behaviors with the risks of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behaviors. Should suicidal thoughts and behaviors emerge during treatment, consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Withdrawal of Antiepileptic Drugs: As with most AEDs, FINTEPLA should generally be withdrawn gradually because of the risk of increased seizure frequency and status epilepticus. If withdrawal is needed because of a serious adverse reaction, rapid discontinuation can be considered.
Serotonin Syndrome: Serotonin syndrome, a potentially life-threatening condition, may occur with FINTEPLA, particularly during concomitant administration of FINTEPLA with other serotonergic drugs, including, but not limited to, selective serotonin-norepinephrine reuptake inhibitors (SNRIs), selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants (TCAs), bupropion, triptans, dietary supplements (eg, St. John’s Wort, tryptophan), drugs that impair metabolism of serotonin (including monoamine oxidase inhibitors [MAOIs], which are contraindicated with FINTEPLA), dextromethorphan, lithium, tramadol, and antipsychotics with serotonergic agonist activity. Patients should be monitored for the emergence of signs and symptoms of serotonin syndrome, which include mental status changes (eg, agitation, hallucinations, coma), autonomic instability (eg, tachycardia, labile blood pressure, hyperthermia), neuromuscular signs (eg, hyperreflexia, incoordination), and/or gastrointestinal symptoms (eg, nausea, vomiting, diarrhea). If serotonin syndrome is suspected, treatment with FINTEPLA should be stopped immediately and symptomatic treatment should be started.
Increase in Blood Pressure: FINTEPLA can cause an increase in blood pressure. Rare cases of significant elevation in blood pressure, including hypertensive crisis, has been reported in adult patients treated with fenfluramine, including patients without a history of hypertension. In clinical trials for DS and LGS of up to 3 years in duration, no pediatric or adult patient receiving FINTEPLA developed hypertensive crisis. Monitor blood pressure in patients treated with FINTEPLA.
Glaucoma: Fenfluramine can cause mydriasis and can precipitate angle closure glaucoma. Consider discontinuing treatment with FINTEPLA in patients with acute decreases in visual acuity or ocular pain.
ADVERSE REACTIONS
The most common adverse reactions observed in DS studies (incidence at least 10% and greater than placebo) were decreased appetite, somnolence, sedation, lethargy, diarrhea, constipation, abnormal echocardiogram, fatigue, malaise, asthenia, ataxia, balance disorder, gait disturbance, increased blood pressure, drooling, salivary hypersecretion, pyrexia, upper respiratory tract infection, vomiting, decreased weight, fall, and status epilepticus.
The most common adverse reactions observed in the LGS study (incidence at least 10% and greater than placebo) were diarrhea, decreased appetite, fatigue, somnolence, vomiting.
DRUG INTERACTIONS
Strong CYP1A2, CYP2B6, or CYP3A Inducers: Coadministration with strong CYP1A2, CYP2B6, or CYP3A inducers will decrease fenfluramine plasma concentrations. If coadministration of a strong CYP1A2, CYP2B6, or CYP3A inducer with FINTEPLA is necessary, monitor the patient for reduced efficacy and consider increasing the dosage of FINTEPLA as needed. If a strong CYP1A2, CYP2B6, or CYP3A inducer is discontinued during maintenance treatment with FINTEPLA, consider gradual reduction in the FINTEPLA dosage to the dose administered prior to initiating the inducer.
Strong CYP1A2 or CYP2D6 Inhibitors: Coadministration with strong CYP1A2 or CYP2D6 inhibitors will increase fenfluramine plasma concentrations. If FINTEPLA is coadministered with strong CYP1A2 or CYP2D6 inhibitors, the maximum daily dosage of FINTEPLA is 20 mg. If a strong CYP1A2 or CYP2D6 inhibitor is discontinued during maintenance treatment with FINTEPLA, consider gradual increase in the FINTEPLA dosage to the dose recommended without CYP1A2 or CYP2D6 inhibitors. If FINTEPLA is coadministered with stiripentol and a strong CYP1A2 or CYP2D6 inhibitor, the maximum daily dosage of FINTEPLA is 17 mg.
USE IN SPECIFIC POPULATIONS
In patients with severe impairment of kidney function (estimated glomerular filtration rate [eGFR]) 15 to 29 mL/min/1.73m2, dosage adjustments are recommended. FINTEPLA has not been studied in patients with kidney failure (eGFR <15 mL/min/1.73m2).
Combined molar exposures of fenfluramine and norfenfluramine were increased in subjects with various degrees of hepatic impairment (Child-Pugh Class A, B, and C), necessitating a dosage adjustment in these patients.
To report SUSPECTED ADVERSE REACTIONS, contact UCB, Inc. at 1-844-599-2273 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see full Prescribing Information, including Boxed Warning and Medication Guide, for additional Important Safety Information on FINTEPLA.
Important Safety Information about BRIVIACT® (brivaracetam) CV in the US2
BRIVIACT® (brivaracetam) CV is indicated for the treatment of partial-onset seizures in patients 1 month of age and older.
WARNINGS AND PRECAUTIONS
Suicidal Behavior and Ideation: Antiepileptic drugs, including BRIVIACT, increase the risk of suicidal behavior and ideation. Monitor patients taking BRIVIACT for the emergence or worsening of depression; unusual changes in mood or behavior; or suicidal thoughts, behavior, or self-harm. Advise patients, their caregivers, and/or families to be alert for these behavioral changes and report them immediately to a healthcare provider.
Neurological Adverse Reactions: BRIVIACT causes somnolence, fatigue, dizziness, and disturbance in coordination. Monitor patients for these signs and symptoms and advise them not to drive or operate machinery until they have gained sufficient experience on BRIVIACT.
Psychiatric Adverse Reactions: BRIVIACT causes psychiatric adverse reactions, including non-psychotic and psychotic symptoms in adult and pediatric patients. Advise patients to report these symptoms immediately to a healthcare provider.
Hypersensitivity: BRIVIACT can cause hypersensitivity reactions. Bronchospasm and angioedema have been reported. Discontinue BRIVIACT if a patient develops a hypersensitivity reaction after treatment. BRIVIACT is contraindicated in patients with a prior hypersensitivity reaction to brivaracetam or any of the inactive ingredients.
Withdrawal of Antiepileptic Drugs: As with all antiepileptic drugs, BRIVIACT should generally be withdrawn gradually because of the risk of increased seizure frequency and statusnepilepticus.
DOSING CONSIDERATIONS
Dose adjustments are recommended for patients with all stages of hepatic impairment.
When BRIVIACT is co-administered with rifampin, an increase in the BRIVIACT dose is recommended.
ADVERSE REACTIONS
In adult adjunctive therapy placebo-controlled clinical trials, the most common adverse reactions (at least 5% for BRIVIACT and at least 2% more frequently than placebo) were somnolence and sedation, dizziness, fatigue, and nausea and vomiting symptoms. Adverse reactions reported in clinical studies of pediatric patients were generally similar to those in adult patients. Adverse reactions with BRIVIACT injection in adult and pediatric patients were generally similar to those observed with BRIVIACT tablets. Other adverse events that occurred in adult patients who received BRIVIACT injection included dysgeusia, euphoric mood, feeling drunk, and infusion site pain.
BRIVIACT is a Schedule V controlled substance.
Please refer to the full Prescribing Information and visit www.BRIVIACThcp.com.
Important Safety Information about VIMPAT® (lacosamide) CV in the US3
VIMPAT is indicated for treatment of partial-onset seizures in patients 1 month of age and older, and as an adjunctive therapy in the treatment of primary generalized tonic-clonic seizures in patients 4 years of age and older.
VIMPAT IMPORTANT SAFETY INFORMATION
VIMPAT is associated with important warnings and precautions including suicidal behavior and ideation, dizziness and ataxia, cardiac rhythm and conduction abnormalities, syncope, and Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), also known as multi-organ hypersensitivity.
Partial-Onset Seizures
In the adult adjunctive placebo-controlled trials for partial-onset seizures, the most common adverse reactions (≥10% and greater than placebo) were dizziness, headache, nausea, and diplopia. In the adult monotherapy clinical trial, adverse reactions were generally similar to those observed and attributed to drug in adjunctive placebo-controlled trials, with the exception of insomnia (observed at a higher rate of ≥2%). Pediatric adverse reactions were similar to those seen in adult patients.
Primary Generalized Tonic-Clonic Seizures
In the adjunctive therapy placebo-controlled trial for primary generalized tonic-clonic seizures, the adverse reactions were generally similar to those that occurred in the partial-onset seizures trials. The adverse reactions most commonly reported were dizziness, somnolence, headache, and nausea.
VIMPAT (lacosamide) is a Schedule V controlled substance.
Please refer to the full Prescribing Information.
References:
- Fintepla® US PI. FINTEPLA (fenfluramine) oral solution: U.S. prescribing information. Smyrna, GA: UCB, Inc.
- BRIVIACT (brivaracetam) prescribing information. Smyrna, GA: UCB, Inc.
- VIMPAT (lacosamide): US prescribing information. Smyrna, GA: UCB, Inc.
- UCB acquires Engage Therapeutics: Staccato® Alprazolam - A potential solution for acute on-demand seizure management for people living with epilepsy. https://www.ucb.com/stories-media/Press-Releases/article/UCB-acquires- Engage-Therapeutics-Staccato-Alprazolam-A-potential-solution-for-acute-on-demand-seizure-management-for-people- living-with-epilepsy. Accessed November 2024.
- Nabbout R, et al. 2024. AES. Poster number 1.401.
- Lhatoo SD, et al. 2024. AES. Poster number 2.388.
- Guerrini R, et al. 2024. AES. Poster number 1.341.
- Lagae L, et al. 2024. AES. Poster number 1.336.
- Nabbout R, et al. 2024. AES. Poster number 1.408.
- Sullivan J, et al. 2024. AES. Poster number 2.393.
- Knupp KG, et al. 2024. AES. Poster number 2.253.
- Bass A, et al. 2024. AES. Poster number 1.501.
- Bailey L, et al. 2024. AES. Poster number 1.498.
- Kaye D, et al. 2024. AES. Poster number 1.100.
- Pathmanathan J, et al. 2024. AES. Poster number 1.521.
- Wittevrongel B, et al. 2024. AES. Poster number 1.530.
- Dedeurwaerdere, et al. 2024. AES. Poster number 1.510.
- Baker GA, et al. 2024. AES. Poster number 2.284.
- Daniels T, et al. 2024. Poster number 3.404.
- Rodriguez-Alvarez N, et al. 2024. AES. Poster number 3.231.
- Gomes AR, et al. 2024. AES. Poster number 3.207.
- Geraerts M, et al. 2024. AES. Poster number 3.202.
- Marra V, et al. 2024. AES. Poster number 1.282.
- Vila Verde D, et al. 2024. AES. Poster number 3.073.
- André VM, et al. 2024. AES. Poster number 3.083.
- Liogier d’Ardhuy X, et al. AES. Poster number 3.109.
- Strzelczyk A, et al. 2024. AES. Poster number 1.344.
- Ameen R, et al. 2024. AES. Poster number 1.499.
- Zhang Roper R, et al. 2024. AES. Poster number 1.497.
- Lagae L, et al. 2024. AES. Poster number 2.362.
- Usui N, et al. 2024. AES. Poster number 3.408.
- Fujimoto A, et al. 2024. AES. Poster number 3.409.
- Hirsch E, et al. 2024. AES. Poster number 2.239.
- Bourikas D, et al. 2024. AES. Poster number 2.386.
- Besson H, et al. 2024. AES. Poster number 2.385.
- Wu X, et al. 2024. AES. Poster number 2.370.
Forward looking statements
This press release may contain forward-looking statements including, without limitation, statements containing the words “believes”, “anticipates”, “expects”, “intends”, “plans”, “seeks”, “estimates”, “may”, “will”, “continue” and similar expressions. These forward-looking statements are based on current plans, estimates and beliefs of management. All statements, other than statements of historical facts, are statements that could be deemed forward-looking statements, including estimates of revenues, operating margins, capital expenditures, cash, other financial information, expected legal, arbitration, political, regulatory or clinical results or practices and other such estimates and results. By their nature, such forward-looking statements are not guarantees of future performance and are subject to known and unknown risks, uncertainties and assumptions which might cause the actual results, financial condition, performance or achievements of UCB, or industry results, to differ materially from those that may be expressed or implied by such forward-looking statements contained in this press release. Important factors that could result in such differences include: the global spread and impact of COVID 19, changes in general economic, business and competitive conditions, the inability to obtain necessary regulatory approvals or to obtain them on acceptable terms or within expected timing, costs associated with research and development, changes in the prospects for products in the pipeline or under development by UCB, effects of future judicial decisions or governmental investigations, safety, quality, data integrity or manufacturing issues; potential or actual data security and data privacy breaches, or disruptions of our information technology systems, product liability claims, challenges to patent protection for products or product candidates, competition from other products including biosimilars, changes in laws or regulations, exchange rate fluctuations, changes or uncertainties in tax laws or the administration of such laws, and hiring and retention of its employees. There is no guarantee that new product candidates will be discovered or identified in the pipeline, will progress to
product approval or that new indications for existing products will be developed and approved. Movement from concept to commercial product is uncertain; preclinical results do not guarantee safety and efficacy of product candidates in humans. So far, the complexity of the human body cannot be reproduced in computer models, cell culture systems or animal models. The length of the timing to complete clinical trials and to get regulatory approval for product marketing has varied in the past and UCB expects similar unpredictability going forward. Products or potential products, which are the subject of partnerships, joint ventures or licensing collaborations may be subject to differences disputes between the partners or may prove to be not as safe, effective or commercially successful as UCB may have believed at the start of such partnership. UCB’s efforts to acquire other products or companies and to integrate the operations of such acquired companies may not be as successful as UCB may have believed at the moment of acquisition. Also, UCB or others could discover safety, side effects or manufacturing problems with its products and/or devices after they are marketed. The discovery of significant problems with a product similar to one of UCB’s products that implicate an entire class of products may have a material adverse effect on sales of the entire class of affected products. Moreover, sales may be impacted by international and domestic trends toward managed care and health care cost containment, including pricing pressure, political and public scrutiny, customer and prescriber patterns or practices, and the reimbursement policies imposed by third-party payers as well as legislation affecting biopharmaceutical pricing and reimbursement activities and outcomes. Finally, a breakdown, cyberattack or information security breach could compromise the confidentiality, integrity and availability of UCB’s data and systems.
Given these uncertainties, you should not place undue reliance on any of such forward-looking statements. There can be no guarantee that the investigational or approved products described in this press release will be submitted or approved for sale or for any additional indications or labelling in any market, or at any particular time, nor can there be any guarantee that such products will be or will continue to be commercially successful in the future.
UCB is providing this information, including forward-looking statements, only as of the date of this press release and it does not reflect any potential impact from the evolving COVID-19 pandemic, unless indicated otherwise. UCB is following the worldwide developments diligently to assess the financial significance of this pandemic to UCB. UCB expressly disclaims any duty to update any information contained in this press release, either to confirm the actual results or to report or reflect any change in its forward-looking statements with regard thereto
or any change in events, conditions or circumstances on which any such statement is based, unless such statement is required pursuant to applicable laws and regulations.
Additionally, information contained in this document shall not constitute an offer to sell or the solicitation of an offer to buy any securities, nor shall there be any offer, solicitation or sale of securities in any jurisdiction in which such offer, solicitation or sale would be unlawful prior to the registration or qualification under the securities laws of such jurisdiction.
BRIVIACT®, FINTEPLA®, and UCBCares® are registered trademarks of the UCB Group of Companies.VIMPAT® is a registered trademark used under license from Harris FRC Corporation. Staccato® is a registered trademark of Alexza Pharmaceuticals, Inc., and is used by UCB Pharma under license.
©2024 UCB, Inc., Smyrna, GA 30080. All rights reserved. US-BR-2400184